Lessons from Ezekiel Emanuel
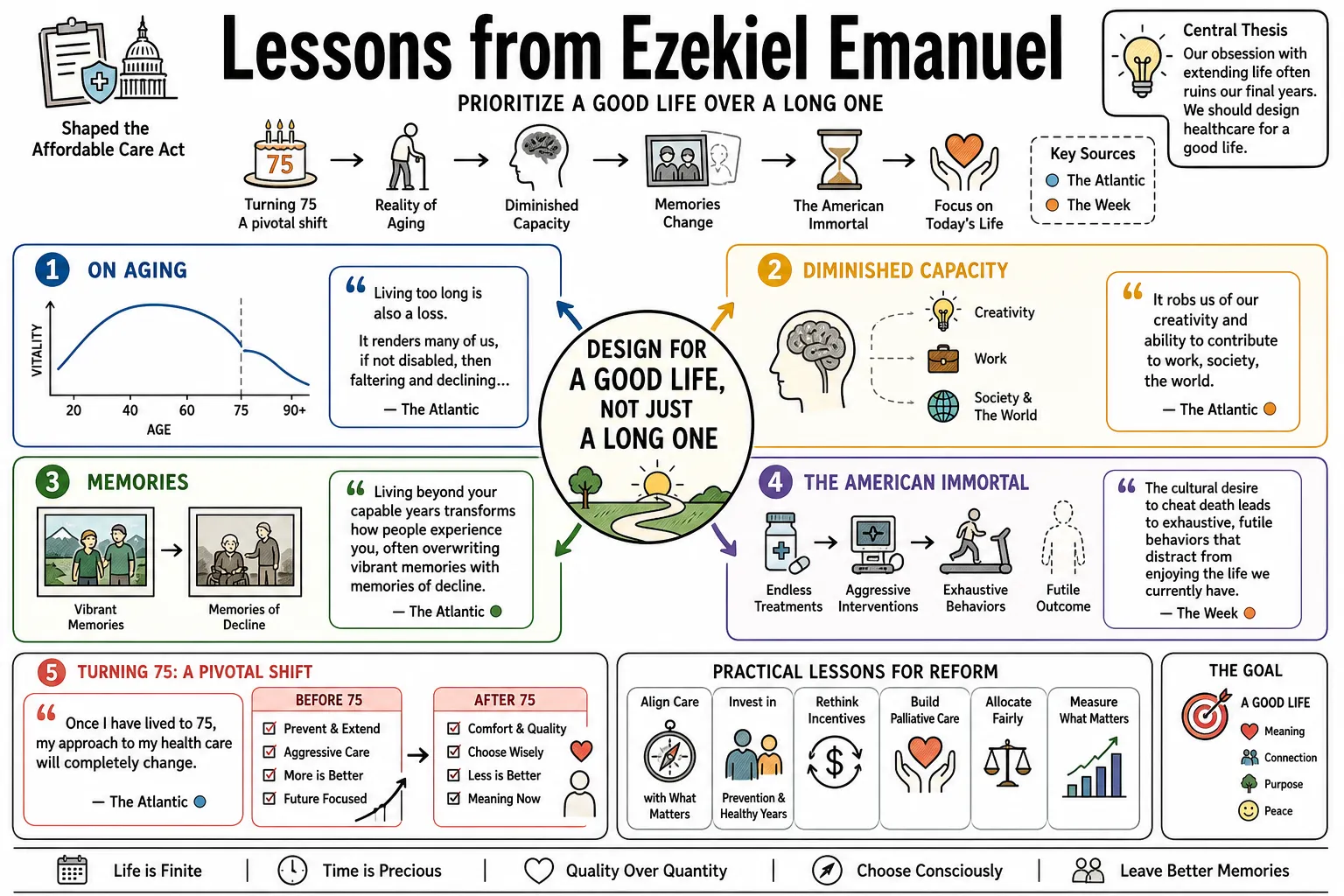
Oncologist and bioethicist Ezekiel Emanuel helped shape the Affordable Care Act and studies how the American medical system functions and fails. He is best known for his essay on hoping to die at 75, which argues that our cultural obsession with extending life often ruins our final years. This collection outlines his practical ideas for reforming healthcare and allocating resources to prioritize a good life over a long one.
Part 1: End-of-Life and Longevity
- On Aging: "Living too long is also a loss. It renders many of us, if not disabled, then faltering and declining..." — Source: The Atlantic
- On Diminished Capacity: "It robs us of our creativity and ability to contribute to work, society, the world." — Source: The Atlantic
- On Memories: Living beyond your capable years transforms how people experience you, often overwriting vibrant memories with memories of decline. — Source: The Atlantic
- On The American Immortal: The cultural desire to cheat death leads to exhaustive, futile behaviors that distract from enjoying the life we currently have. — Source: The Week
- On Turning 75: "Once I have lived to 75, my approach to my health care will completely change. I won't actively end my life. But I won't try to prolong it, either." — Source: The Atlantic
- On Preventative Care in Old Age: After 75, routine medical interventions like cancer screenings and pacemakers shift from life-saving necessities to burdens that merely extend the dying process. — Source: The Atlantic
- On Quality Over Quantity: The goal of medicine should shift from aggressively extending the human lifespan to improving the quality of the years we are naturally given. — Source: ASCO Post
- On Legacy: Society should focus less on keeping the elderly alive and more on ensuring they leave a legacy of contribution and character. — Source: The Atlantic
- On Meaningful Lifespans: "Doubtless, death is a loss. It deprives us of experiences and milestones... But living too long is also a loss." — Source: Johns Hopkins University
- On Personal Choice: Choosing to forego life-extending care at an advanced age is a deeply personal preference, separate from any proposed public policy mandate. — Source: Charlie Doggett Network
Part 2: Wellness and Lifestyle
- On Joie de Vivre: "Wellness should be about joie de vivre — about joy in life. It should not be only self-deprivation." — Source: Retirement Wisdom
- On Common Sense Health: Most wellness advice boils down to avoiding stupid, self-destructive risks instead of discovering complex new biological hacks. — Source: Retirement Wisdom
- On Social Connection: Cultivating family and friendships is as biologically necessary for a long life as diet and exercise. — Source: The Dr. Hyman Show
- On Mental Agility: Expanding your mind through continuous learning is a requirement to stay mentally sharp as the body ages. — Source: The Dr. Hyman Show
- On Dietary Balance: Eat your ice cream. Food should bring joy; moderate indulgence is superior to lifelong dietary obsession. — Source: Big Think
- On Movement: Regular, natural movement outpaces hyper-regimented gym routines for long-term health. — Source: Big Think
- On Sleep: Prioritizing high-quality rest is fundamental, never a luxury to be traded for productivity. — Source: The Dr. Hyman Show
- On Tracking Culture: "The whole book is about stopping obsessed, stopping crazy. Stop tracking everything." — Source: Saga
- On Habituation: Wellness interventions fail if they cannot be maintained as effortless habits over decades. — Source: Saga
- On Phone Metrics: In Health & Veritas, Emanuel says he does not look at phone-based health metrics and avoids tracking steps, sleep, and food; he treats a few cycling numbers as useful feedback, not the center of wellness. — Reference: Yale Health & Veritas transcript with Emanuel on phone metrics and non-obsessive tracking
Part 3: Bioethics and Resource Allocation
- On The Hippocratic Oath: "Doctors take the Hippocratic Oath too seriously, as an imperative to do everything for the patient regardless of the cost or effects on others." — Source: QuoteFancy
- On Resource Limits: Bioethics must grapple with the reality of scarce resources; ignoring cost is a failure of ethical imagination. — Source: FactCheck.org
- On Distributive Justice: Allocating medical care requires balancing individual need against the broader health outcomes of the community. — Source: Time Magazine
- On Futile Care: Pouring infinite resources into medically futile interventions for terminal patients deprives the rest of society of necessary care. — Source: FactCheck.org
- On Patient Autonomy: Autonomy is vital, but it does not entitle patients to demand treatments that are medically unproven or societally ruinous. — Source: UPenn Bioethics
- On Pragmatism in Ethics: Theoretical bioethics often fails at the bedside; ethical guidelines must account for the messy reality of clinical practice. — Source: UPenn Bioethics
- On Defining Value: The value of a medical intervention lies in the concrete improvement it brings to a patient's life, regardless of its technical sophistication. — Source: UPenn Bioethics
- On Pediatric Priority: Society has a heightened moral obligation to invest in the health and development of children over marginal life extensions for the very old. — Source: Time Magazine
- On Shared Decision Making: Medical choices should be a negotiation between a physician's expertise and a patient's values, rejecting top-down directives. — Source: QuoteFancy
- On Moral Hazard: Shielding patients entirely from the cost of their care encourages the overutilization of low-value medical services. — Source: UPenn Bioethics
Part 4: The Affordable Care Act and Health Policy
- On ACA Intent: The Affordable Care Act was designed to aggressively reduce the number of uninsured Americans and correct blatant injustices in coverage. — Source: Health Affairs
- On Pre-existing Conditions: Banning denials for pre-existing conditions was the moral core of the ACA, shifting insurance from risk-selection to actual care. — Source: Reinventing American Health Care
- On System Complexity: "Imagine you were shopping for a new shirt but there was no price tag and you could not know until weeks after you bought it whether the shirt cost $25 or $200." — Source: Goodreads
- On Legislative Compromise: Effective health policy requires accepting imperfect legislation over maintaining a broken status quo. — Source: Washington Post
- On Employer-Sponsored Insurance: The historical accident of tying health insurance to employment remains a central flaw in the American system. — Source: Reinventing American Health Care
- On Healthcare Exchanges: "I believe the majority of private-sector workers will get their coverage through the exchanges." — Source: Goodreads
- On Tax Deductions: Failing to eliminate the tax deduction for employer-provided health benefits was a major missed opportunity of the ACA. — Source: Washington Post
- On Reform Trajectory: The ACA serves as a foundational step that catalyzes necessary long-term changes in care delivery. — Source: UPenn Leonard Davis Institute
- On Political Reality: Health care reform in America involves navigating entrenched corporate interests as much as improving patient health. — Source: Equitable Growth
- On Universal Coverage: Achieving universal coverage is structurally impossible in a purely free-market system without government intervention. — Source: Health Affairs
Part 5: The U.S. Healthcare System's Flaws
- On Waste: The American medical system produces excellent acute interventions but chokes on administrative bloat and redundant testing. — Source: Reinventing American Health Care
- On Pricing Opacity: The inability for patients to know the cost of a procedure beforehand reflects a deliberate failure of the medical market. — Source: Reinventing American Health Care
- On Fee-for-Service: Paying doctors for the volume of procedures they perform guarantees over-treatment and inflated costs. — Source: Prescription for the Future
- On Error Rates: The fragmentation of American healthcare creates dangerous communication gaps, leading to preventable, systemic medical errors. — Source: Reinventing American Health Care
- On Preventative Neglect: The U.S. system is optimized for rescuing people from the brink of death, yet fails at preventing them from getting sick in the first place. — Source: Prescription for the Future
- On Pharmaceutical Pricing: Unchecked drug pricing reflects regulatory capture and monopoly power, independent of actual research costs. — Source: Prescription for the Future
- On Hospital Monopolies: When hospital systems consolidate, the primary result is higher prices for local patients with little improvement to clinical outcomes. — Source: Health Affairs
- On End-of-Life Spending: The vast sums spent in the last months of a patient's life often cause active suffering with zero clinical benefit. — Source: Reinventing American Health Care
- On Outlier Spending: A massive percentage of healthcare spending is driven by a tiny fraction of chronically ill patients who require coordinated, VIP-level care management. — Source: Prescription for the Future
Part 6: Healthcare Megatrends and The Future
- On Hospital Contraction: The future of medicine involves a drastic reduction in hospital beds as care moves into the home and outpatient centers. — Source: University of Kentucky
- On VIP Care Models: The system must pivot to provide high-touch, coordinated care specifically for the chronically and mentally ill to reduce overall costs. — Source: Prescription for the Future
- On Insurance Evolution: Insurance companies will survive only by transforming from claims processors into predictive analytics and service-oriented firms. — Source: University of Kentucky
- On Digital Medicine: Telehealth and remote monitoring are permanent foundations for future chronic disease management, independent of pandemic constraints. — Source: In the Bubble Podcast
- On Value-Based Care: The shift from volume-based billing to value-based care is inevitable and forces providers to guarantee outcomes. — Source: Prescription for the Future
- On Behavioral Economics: Successfully changing patient and physician behavior requires understanding economics and cognitive biases. — Source: Prescription for the Future
- On Mental Health Integration: Treating behavioral health as distinct from physical health is a clinical failure; the two must be integrated at the primary care level. — Source: Prescription for the Future
- On Data Interoperability: A functional healthcare future relies on systems that can talk to one another, ending the era of siloed electronic health records. — Source: In the Bubble Podcast
- On the End of Solo Practice: The complexity of modern medicine and billing effectively ends the solo physician practice in favor of large, integrated groups. — Source: Prescription for the Future
Part 7: The Medical Profession and Physician Duty
- On Physician Burnout: Burnout is often a structural issue caused by administrative friction and broken software, distinct from a lack of physician resilience. — Source: Prescription for the Future
- On Training Doctors: Medical education must shift from memorizing biological facts to understanding health systems, data analytics, and team-based care. — Source: UPenn Medical Ethics
- On Palliative Care: Palliative medicine should be introduced at the moment of a serious diagnosis; delaying it until the final days of life is a clinical failure. — Source: UPenn Medical Ethics
- On Hubris: Physicians often confuse their technical ability to intervene with a moral imperative to do so. — Source: The Atlantic
- On Listening: The most effective, lowest-cost diagnostic tool in medicine remains taking an unhurried, careful history from the patient. — Source: UPenn Medical Ethics
- On Malpractice Fear: The practice of defensive medicine harms patients physically and bankrupts the system financially. — Source: Reinventing American Health Care
- On Team-Based Care: The lone doctor is a myth; effective modern healthcare requires integrated teams of nurses, pharmacists, and social workers. — Source: Prescription for the Future
- On Empathy: Medical technology can cure, but healing requires human empathy, a quality constantly strained by the demands of the modern clinic. — Source: UPenn Medical Ethics
- On Financial Transparency: Doctors have an ethical duty to consider the financial toxicity of the treatments they prescribe to their patients. — Source: Prescription for the Future
Part 8: Public Health, Pandemics, and Vaccines
- On COVID-19 Response: "It's shocking. It's horrible. The United States really has done remarkably badly compared to other countries." — Source: Wikiquote
- On Vaccine Value: "Vaccines are the most cost-effective health care interventions there are. A dollar spent on a childhood vaccination not only helps save a life, but greatly reduces spending on future healthcare." — Source: QuoteFancy
- On Public Health Underfunding: The chronic underfunding of local public health departments leaves the nation perpetually vulnerable to novel biological threats. — Source: On with Kara Swisher
- On Global Health: Pandemics do not respect borders; global health security demands international cooperation and vaccine equity. — Source: On with Kara Swisher
- On Science Communication: Public health officials must communicate risk with absolute clarity and humility, admitting openly when data changes. — Source: On with Kara Swisher
- On Individual Mandates: Public health occasionally requires limiting individual freedoms to protect the vulnerable from communicable diseases. — Source: UPenn Medical Ethics
- On Institutional Trust: The politicization of public health agencies during crises causes lasting damage that outlives the immediate pathogen. — Source: In the Bubble Podcast
- On Preparation: Reacting to a pandemic after community spread has begun is a failure; true biodefense relies on early detection and rapid, coordinated action. — Source: In the Bubble Podcast