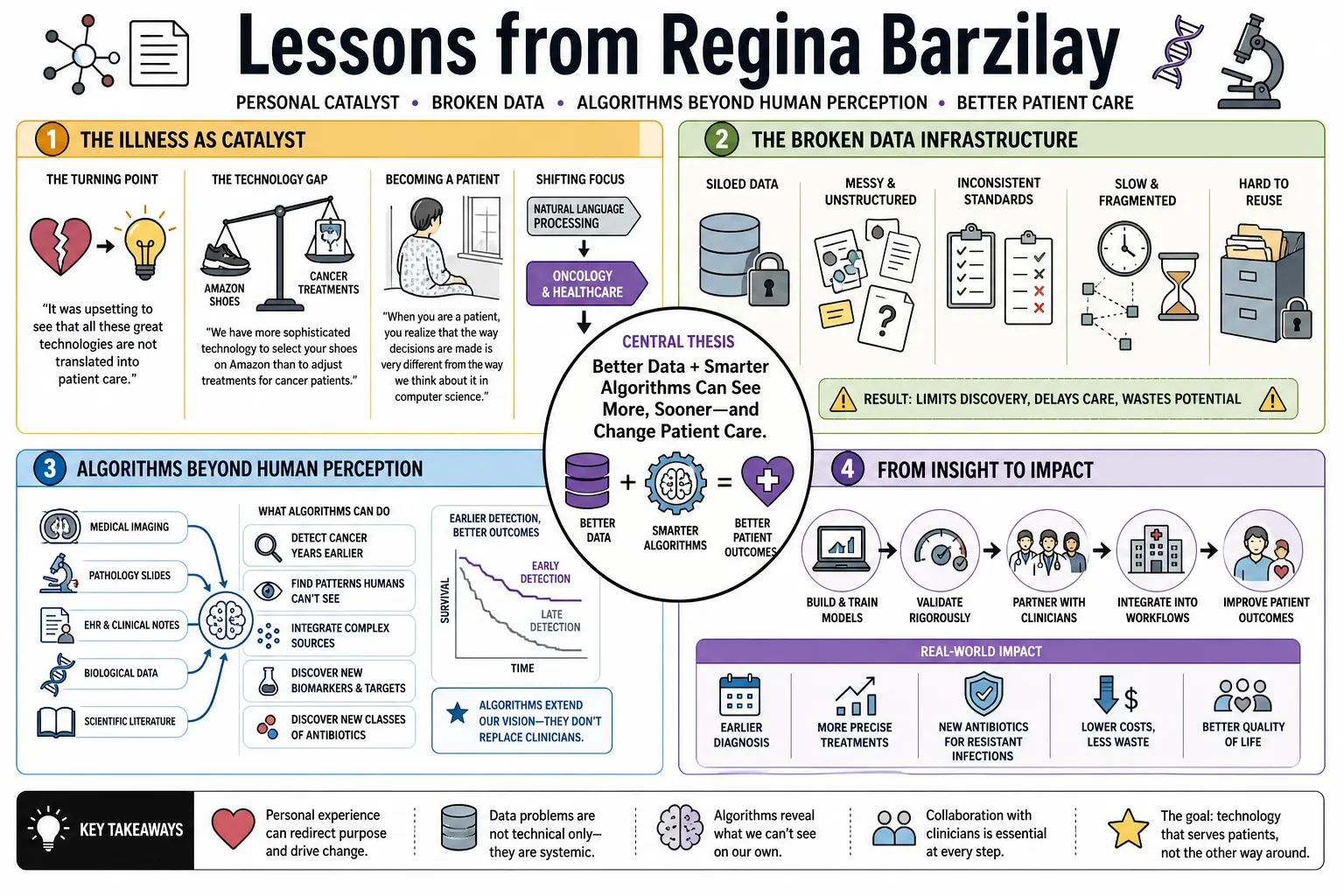
After her own breast cancer diagnosis, MIT computer scientist Regina Barzilay redirected her research from natural language processing to healthcare. She builds machine learning models that spot cancer years before doctors can and discover entirely new classes of antibiotics. This collection outlines her views on medicine's broken data infrastructure and how algorithms can bypass the limits of human perception to change patient care.
Part 1: The Illness as Catalyst
- On the turning point: "It was upsetting to see that all these great technologies are not translated into patient care. I wanted to change it." — Source: [MIT Jameel Clinic]
- On the technology gap: "Going through it, I realized that today we have more sophisticated technology to select your shoes on Amazon than to adjust treatments for cancer patients." — Source: [Lex Fridman Podcast]
- On becoming a patient: "When you are a patient, you realize that the way decisions are made is very different from the way we think about it in computer science. It’s not always data-driven." — Source: [Lex Fridman Podcast]
- On shifting focus: She redirected her entire career from natural language processing to oncology because she recognized that the machine learning tools she built for text were desperately needed to save lives in clinical settings. — Source: [MacArthur Foundation]
- On the motivation to build: The drive to develop predictive AI models came directly from a desire to bring the power of existing clinical data to doctors, helping them make more informed, concrete decisions. — Source: [Lex Fridman Podcast]
- On the reality of care: Experiencing treatment firsthand exposed how much of clinical practice relies on manual interpretation and historical intuition rather than rigorous, individualized data analysis. — Source: [WebMD]
- On missing the obvious: She saw that massive amounts of medical imaging and records were being stored but functionally ignored by a system not equipped to extract deeper patterns. — Source: [PBS Nova]
- On the goal of her lab: "My goal is to bring the power of the data we already have to help doctors make better decisions." — Source: [Lex Fridman Podcast]
- On actionable data: The frustration of a patient is realizing the answer might exist in a database, but the hospital lacks the infrastructure to retrieve and apply it to their specific case. — Source: [Science Media Hub]
- On personal stakes: Her diagnosis in 2014 was not just a health crisis; it was an empirical observation of a broken system that she possessed the exact technical skills to begin fixing. — Source: [Wikipedia]
Part 2: Rethinking Early Detection
- On personalized screening: "We cannot create a dress that is going to fit everybody: you really need to have a dress that is based on your individual body." — Source: [National Academy of Medicine]
- On the goal of prediction: "We want to answer questions like: how much earlier can you predict that somebody is going to develop cancer? For breast cancer, we already demonstrated that you can do that quite well." — Source: [Science Media Hub]
- On shifting timelines: "My personal bet is that within a few years, the stage of diagnosis across many cancers will come much earlier than we are heading." — Source: [BBC]
- On targeted screening: "With this kind of technology, you would be able to identify who really needs to be screened because of course we don't want to overscreen." — Source: [BBC]
- On changing clinical trials: "The hope is that if you can predict, very early on, that the patient is in the wrong way, you can do clinical trials, you can develop the drugs that are doing the prevention, rather than treatment of very advanced disease." — Source: [WebMD]
- On the Mirai model: Her algorithm was designed to predict breast cancer risk up to five years in advance by analyzing mammograms for patterns that precede visible tumors. — Source: [MIT News]
- On the Sybil model: For lung cancer, her team built a model that analyzes low-dose CT scans to predict disease development within six years, identifying risk in scans doctors would classify as completely normal. — Source: [MIT News]
- On outdated standards: She recognized that traditional risk models like Tyrer-Cuzick rely on rudimentary demographic factors, failing to utilize the rich, patient-specific data contained within a single medical image. — Source: [National Academy of Medicine]
- On prevention vs. treatment: The ultimate utility of AI in oncology is moving the timeline backward, shifting medical intervention from aggressive late-stage treatment to early-stage prevention. — Source: [The Economist]
- On validating models: True predictive models must prove their efficacy not just in a lab, but by matching their forecasts against years of historical patient follow-up data across multiple hospitals. — Source: [Science Media Hub]
Part 3: Transcending Human Perception
- On human visual limits: "As a human, we cannot really do this because our capacity to see things is limited." — Source: [WebMD]
- On machine vision: "But a machine can capture much more subtle patterns because it looks at all these pixels and has much better ability than our eyes." — Source: [WebMD]
- On the Achilles heel of diagnosis: The reliance on the human eye to spot visible masses means the disease has often been developing for years before a radiologist can physically see it. — Source: [National Academy of Medicine]
- On complex correlations: Machines excel where humans fail because they can capture complicated, microscopic correlations in tissue density that correspond to future cancer growth. — Source: [WebMD]
- On sub-perceptual patterns: AI models are trained to identify subtle harbingers of disease that exist in the pixel data but register as completely invisible to even the most trained medical professionals. — Source: [PBS Nova]
- On predictive training: By feeding models hundreds of thousands of images paired with long-term patient outcomes, the algorithm learns what healthy tissue looks like right before it turns malignant. — Source: [National Academy of Medicine]
- On redefining normal: A scan that a human radiologist clears as normal often contains latent structural information that a machine can interpret as a high-risk trajectory. — Source: [PBS Nova]
- On algorithmic advantage: We require humans to have clear, recognizable patterns to make a diagnosis, while AI can aggregate thousands of slight deviations into a definitive risk profile. — Source: [WebMD]
- On human-machine roles: The goal is not to replace the radiologist's ability to see a tumor, but to provide them with a tool that sees what precedes the tumor. — Source: [PBS Nova]
Part 4: AI in Drug Discovery
- On finding compounds: "If discovering new drugs is like searching for a needle in a haystack, AI acts like a metal detector." — Source: [Verseon]
- On a historic first: The discovery of Halicin represented the first time a completely new antibiotic was identified using a machine-learning model that assessed molecular patterns independently of human intuition. — Source: [The Guardian]
- On zooming in: She describes AI as a tool capable of instantly zooming in on a fruitful set of hypotheses that human researchers could miss for decades. — Source: [The Guardian]
- On structural training: Her team trained a neural network on 2,500 molecules, teaching it to predict which chemical structures would successfully inhibit the growth of bacteria like E. coli. — Source: [Cell]
- On screening scale: Once trained, the algorithm screened a library of over 6,000 compounds in a fraction of the time it would take human researchers to test them manually. — Source: [MIT News]
- On breaking conventions: The AI identified a molecule—originally tested for diabetes—that possessed a chemical structure entirely unlike any known antibiotic class. — Source: [Quanta Magazine]
- On biological mechanisms: Halicin proved effective because it disrupts the proton motive force of bacteria, a fundamental energy process that makes it incredibly difficult for the bacteria to develop resistance. — Source: [Cell]
- On the naming convention: The team named the new antibiotic Halicin as a direct homage to HAL 9000, acknowledging the central role artificial intelligence played in its discovery. — Source: [MIT News]
- On repurposing drugs: AI accelerates timelines not just by finding new molecules, but by identifying hidden, secondary uses for drugs that have already passed initial safety trials in humans. — Source: [WBUR]
- On the post-antibiotic era: Deploying machine learning to find novel bacterial inhibitors is a necessary defense strategy as traditional antibiotics rapidly lose their efficacy against resistant strains. — Source: [Calcalistech]
Part 5: The Healthcare Data Deficit
- On commercial priorities: "We have better databases for movies and shopping than we have for healthcare." — Source: [ODSC]
- On privacy as a barrier: "Of course there are concerns about patient data privacy, but there are so many patients whose disease became so much more severe because it was not detected early enough." — Source: [Science Media Hub]
- On balancing risk: "We have to find a way to balance data privacy with the need for much larger databases." — Source: [Science Media Hub]
- On the missing foundation: The lack of standardized, easily accessible healthcare databases remains the primary hurdle preventing life-saving AI models from reaching their full potential. — Source: [ODSC]
- On the unbridgeable gap: She frequently highlights the travesty of living in a data-rich technological era while clinical practice remains comparatively data-poor due to siloed information. — Source: [MIT News]
- On extracting unstructured data: A massive portion of medical insight is trapped in unstructured clinical notes and pathology reports, requiring advanced natural language processing to make it useful. — Source: [ACM ByteCast]
- On the cost of caution: Protecting privacy at the absolute expense of data sharing directly results in worse patient outcomes by starving research of the information needed to spot trends. — Source: [Science Media Hub]
- On systemic lag: The medical profession remains behind the curve on AI integration primarily because its data infrastructure was built for billing and compliance, not machine learning. — Source: [Brave New World Podcast]
- On redefining infrastructure: Moving beyond incremental clinical improvements requires fundamentally rethinking how hospitals curate, store, and share patient data across the healthcare ecosystem. — Source: [TechBio Talks]
Part 6: Confronting Bias and Equity
- On baseline reality: "There is a lot of bias and inequality in medicine, period." — Source: [Ynetnews]
- On inherited prejudice: Algorithms can inherit our own biases when they are trained on observational datasets that reflect the unequal treatment decisions of human providers. — Source: [MIT News]
- On data representation: Biased predictive models are almost always the direct result of the distributional properties of the training data, where underrepresented populations are ignored. — Source: [MIT News]
- On the perfect world fallacy: We are not bringing AI to a perfect world; the standard we compare AI against is a flawed human system that already relies on racially biased tools. — Source: [The Media Line]
- On leveling the field: Properly trained AI has the unique ability to standardize high-quality diagnostics, ensuring a rural clinic has the same analytical power as an elite research hospital. — Source: [MIT News]
- On global validation: To prevent bias, her team rigorously tested the Mirai risk model across diverse global populations to ensure its accuracy held up across different races and ethnicities. — Source: [Ynetnews]
- On clinical inequity: Human clinicians routinely offer different treatment plans based on a patient's socioeconomic status; AI models must be explicitly designed to ignore these historical prejudices. — Source: [ACM ByteCast]
- On auditing algorithms: Because machine learning models are mathematical, we can audit them for bias much more rigorously than we can audit the private thought processes of human doctors. — Source: [MIT News]
- On improving upon humans: The goal of clinical AI is not to perfectly mimic human doctors, but to explicitly remove the human biases that have historically degraded the quality of care for minorities. — Source: [The Media Line]
Part 7: Deciphering Language and Texts
- On ancient text translation: "Traditionally, decipherment has been viewed as a sort of scholarly detective game, and computers weren't thought to be of much use." — Source: [National Geographic]
- On modern methodology: "Our aim is to bring to bear the full power of modern machine learning and statistics to this problem." — Source: [National Geographic]
- On computational efficiency: The output of our system would have made the process orders of magnitude shorter, bypassing the years of manual work and happy coincidences required by early linguists. — Source: [MIT News]
- On human-AI collaboration: AI is not designed to replace linguists but acts as a powerful statistical tool that can rapidly corroborate relationships between complex language families. — Source: [MIT News]
- On linguistic peculiarities: "Each language has its own challenges. Most likely, a successful decipherment would require one to adjust the method for the peculiarities of a language." — Source: [MIT News]
- On the Ugaritic breakthrough: Her algorithm correctly mapped 29 of the 30 letters in the lost Ugaritic alphabet in a matter of hours by comparing its structure to Hebrew. — Source: [MIT News]
- On mapping relationships: She built systems capable of verifying that languages like Iberian are not related to Basque, operating entirely without a parallel text or Rosetta Stone. — Source: [MIT News]
- On text summarization: Before her work in healthcare, she pioneered algorithms capable of processing massive volumes of distinct documents and distilling them into coherent, single-text summaries. — Source: [MacArthur Foundation]
- On language grounding: She advanced reinforcement learning techniques that successfully mapped abstract natural language commands to physical actions within simulated environments. — Source: [MacArthur Foundation]
Part 8: Bridging the Translation Gap
- On ubiquitous application: "Today almost every aspect of our life is driven by machine learning predictions – be it travel, banking or entertainment." — Source: [Abdul Latif Jameel]
- On the healthcare exception: "The only area where we do not benefit from this powerful technology is the one which impacts us the most, our healthcare." — Source: [Abdul Latif Jameel]
- On the mission of Jameel Clinic: "We aim to bring the best of AI technology we develop in our labs at MIT to hospitals and clinics in the United States and around the world." — Source: [Abdul Latif Jameel]
- On academic limits: Publishing an algorithmic breakthrough in a computer science journal is meaningless in healthcare if the tool is never integrated into a doctor's actual daily workflow. — Source: [Open Data Science]
- On seamless integration: For medical AI to be effective, it cannot be a separate software application a doctor has to open; it must provide seamless, automated support within existing hospital systems. — Source: [Open Data Science]
- On interdisciplinary teams: Solving the translation gap requires programmers to sit directly alongside doctors and lawyers, ensuring the technology respects both clinical realities and regulatory constraints. — Source: [Brave New World Podcast]
- On changing the standard of care: The ultimate measure of success for medical AI is not predictive accuracy on a historical dataset, but whether it actively alters the standard of care for future patients. — Source: [ACM ByteCast]
- On the future of diagnosis: She envisions a near-term reality where every patient scan is automatically reviewed by an AI layer that flags predictive risks before a human specialist ever sees the image. — Source: [Lex Fridman Podcast]
- On the urgency of deployment: The cost of delaying AI implementation in clinical settings is measured in preventable late-stage diagnoses and lost lives. — Source: [Science Media Hub]