Lessons from Shiv Rao
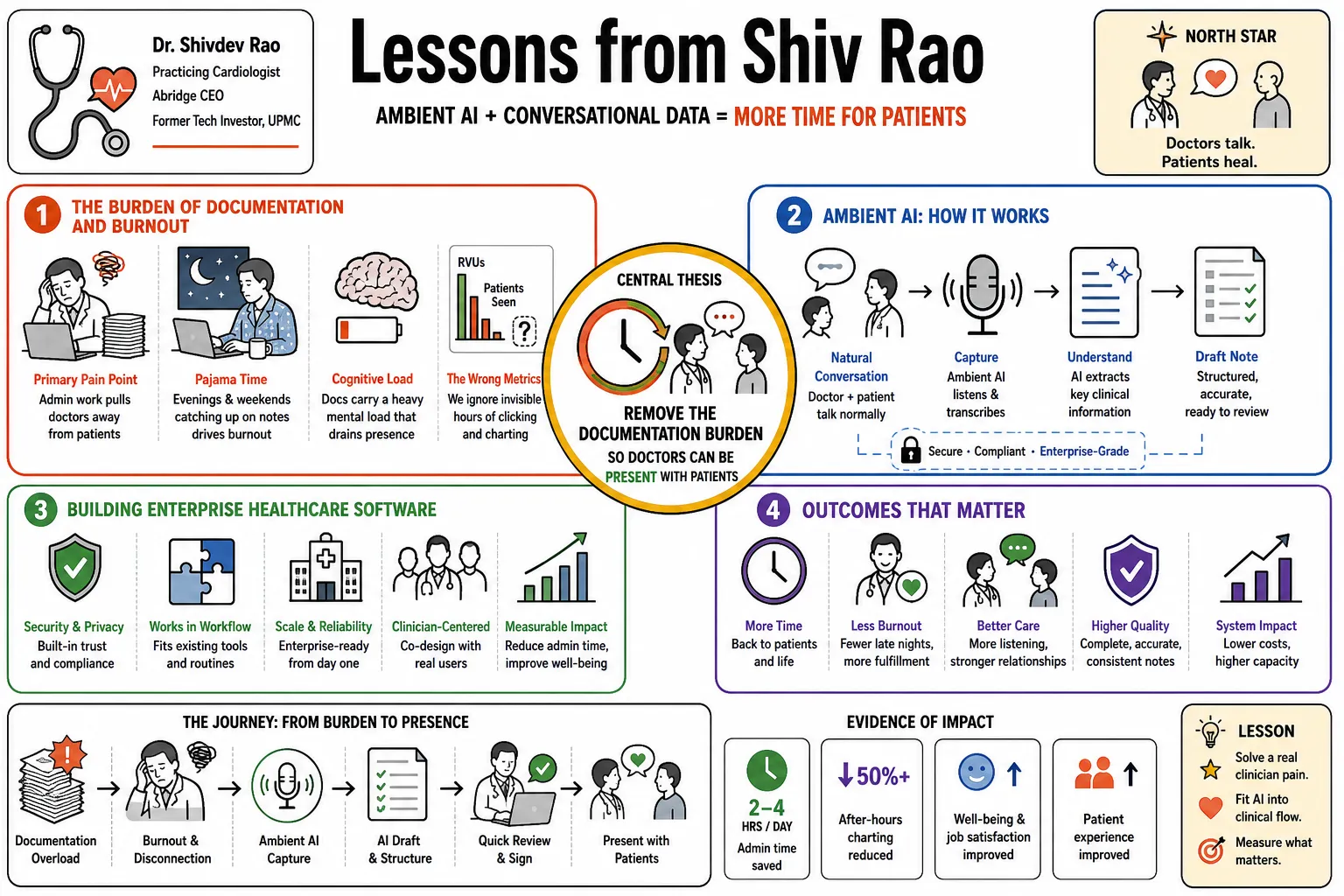
Practicing cardiologist and Abridge CEO Dr. Shivdev Rao builds ambient clinical documentation software to cut the data-entry work that drives clinician burnout. Drawing on his experience treating patients and managing tech investments at UPMC, he explains how to build enterprise healthcare software and fit AI into clinical routines. This profile collects his advice on using conversational data to give doctors more time to actually talk to their patients.
Part 1: The Burden of Documentation and Burnout
- On the primary pain point: "The most pressing issue in medicine today isn't a lack of clinical knowledge, it's the crushing weight of administrative tasks that take doctors away from patients." — Source: [NEJM AI Grand Rounds]
- On pajama time: "Physicians are spending their evenings and weekends catching up on notes. That 'pajama time' is the single biggest driver of burnout across the industry." — Source: [The Heart of Healthcare]
- On cognitive load: "Documentation isn't just time-consuming; it carries a massive cognitive load that drains a doctor's ability to be fully present." — Source: [No Priors Podcast]
- On the wrong metrics: "We often measure productivity by RVUs or patients seen, but we ignore the invisible hours spent clicking through an EHR after the clinic closes." — Source: [The 20 Minute VC]
- On retaining talent: "If we don't solve the documentation burden, we will continue to lose some of our brightest and most compassionate clinicians to early retirement." — Source: [Digital Health Inside Out]
- On systemic failure: "Burnout is frequently framed as an individual resilience problem, but it is fundamentally a systems failure caused by broken software workflows." — Source: [Observer Interview]
- On physician well-being: "You cannot deliver exceptional patient care if the person delivering that care is chronically exhausted from data entry." — Source: [The Heart of Healthcare]
- On the goal of technology: "Technology in the exam room should serve as a shock absorber for the clinician's administrative burden, rather than an amplifier." — Source: [Health Evolution]
- On the hidden cost of care: "The time spent documenting is the unbilled, unappreciated tax that every medical professional pays daily." — Source: [This Week in Startups]
- On shifting focus: "When you remove the two hours of documentation at the end of the day, you give a clinician their life back." — Source: [Pioneers of AI]
Part 2: Restoring the Human Connection in Care
- On the core of medicine: "The most valuable diagnostic tool we have is the conversation between a patient and their doctor." — Source: [HLTH Conference]
- On eye contact: "Patients notice when their doctor is staring at a screen instead of looking them in the eye. That subtle shift degrades trust." — Source: [NEJM AI Grand Rounds]
- On empathy at scale: "If we can automate the administrative chores, we effectively scale empathy because we give providers the space to actually listen." — Source: [The 229 Podcast]
- On unmediated interaction: "A doctor should be able to walk into a room, sit down, and simply talk to the person in front of them without a keyboard in the way." — Source: [Abridge Blog]
- On active listening: "When you don't have to worry about memorizing what to type later, you transition from a data gatherer back to an active listener." — Source: [The Heart of Healthcare]
- On the art of healing: "Medicine is part science and part art, and the art lives entirely in the human connection that happens in the clinic." — Source: [No Priors Podcast]
- On patient understanding: "A well-documented conversation doesn't just help the doctor; it helps the patient remember and understand their own care plan." — Source: [Digital Health Inside Out]
- On reducing friction: "Every click and keystroke is friction between the provider and the patient. Our job is to eliminate that friction." — Source: [The 20 Minute VC]
- On being present: "Presence cannot be billed, but it is the most critical factor in achieving better health outcomes." — Source: [Observer Interview]
- On returning to roots: "We are using advanced artificial intelligence to bring medicine back to its simplest form: two people talking in a room." — Source: [Pioneers of AI]
Part 3: From Novelty to Conversational Infrastructure
- On AI beyond the scribe: "An AI scribe is just the tip of the spear. The real value is building a conversational intelligence layer for all of healthcare." — Source: [The 229 Podcast]
- On the value of speech: "Speech is the highest bandwidth way we communicate, yet for decades it was the least structured data in the medical record." — Source: [NEJM AI Grand Rounds]
- On party tricks vs. utility: "There is a massive gulf between an AI demo that looks like a neat party trick and a system that actually withstands the rigors of a busy clinic." — Source: [Digital Health Inside Out]
- On computing the conversation: "We are turning the unstructured dialogue of a medical visit into computable infrastructure that can trigger downstream actions." — Source: [No Priors Podcast]
- On note generation: "It was never just about writing the note. The note is simply the first artifact derived from structuring clinical dialogue." — Source: [HLTH Conference]
- On the data exhaust: "The ambient audio of a clinic visit contains rich context that is entirely lost when distilled manually into a dry medical summary." — Source: [The Heart of Healthcare]
- On continuous improvement: "Conversational infrastructure gets smarter with every interaction, creating a compounding advantage for both the software and the user." — Source: [This Week in Startups]
- On moving beyond transcription: "Transcription is a commodity. Understanding the clinical intent behind the words is where the actual hard computer science happens." — Source: [Abridge Blog]
- On system-wide intelligence: "When you capture the conversation accurately, you can begin to automate coding, billing, and follow-up scheduling simultaneously." — Source: [The 20 Minute VC]
- On structural shifts: "We are shifting from a world where doctors translate conversations for computers, to a world where computers translate conversations for doctors." — Source: [Pioneers of AI]
Part 4: Building Enterprise-Grade Healthcare AI
- On model orchestration: "You cannot rely on a single foundational model for everything. Enterprise healthcare requires orchestrating multiple specialized models to handle different facets of clinical reasoning." — Source: [Digital Health Inside Out]
- On edge cases: "In consumer tech, a 95% accuracy rate is phenomenal. In healthcare, that 5% edge case can be a life-altering medical error." — Source: [NEJM AI Grand Rounds]
- On clinical rigor: "Building for the enterprise means proving to chief medical officers that your technology is as rigorous as the medicine they practice." — Source: [The 20 Minute VC]
- On scaling operations: "Scaling an AI solution across a massive health system requires more than good code; it demands an obsessive focus on change management and deployment strategy." — Source: [Health Evolution]
- On latency: "A doctor will not wait thirty seconds for a note to generate. The system has to feel instantaneous to fit into their cognitive flow." — Source: [No Priors Podcast]
- On reliability: "If the AI goes down for an hour in a busy hospital, it causes chaos. Enterprise-grade means absolute reliability." — Source: [The 229 Podcast]
- On adapting to specialties: "A pediatric psychiatry visit sounds fundamentally different than a cardiology follow-up. The AI must be versatile enough to map to any specialty." — Source: [Abridge Blog]
- On audio challenges: "Clinical environments are noisy. Your models have to handle crying babies, background alarms, and multiple people talking over one another." — Source: [This Week in Startups]
- On evaluating models: "We evaluate our models not just on standard benchmarks, but on whether they capture the precise medical reasoning a physician expects to see." — Source: [Observer Interview]
Part 5: Clinical Workflows and EHR Integration
- On integration philosophy: "We shouldn't force doctors to adopt a parallel workflow. Our software must live exactly where they already work." — Source: [Observer Interview]
- On working with Epic: "Partnering deeply with EHR vendors like Epic is essential because that is the central nervous system of the hospital." — Source: [No Priors Podcast]
- On seamless adoption: "The best clinical software requires zero training. A doctor should be able to turn it on and intuitively understand how it helps them." — Source: [Digital Health Inside Out]
- On the last mile: "Generating a great summary is only half the battle. The last mile is routing that structured data into the correct fields within the EHR without manual copy-pasting." — Source: [The 229 Podcast]
- On disruption: "Healthcare doesn't need to be 'disrupted' by outsiders; it needs to be supported by builders who respect the existing clinical workflows." — Source: [HLTH Conference]
- On workflow optimization: "If your tool saves five minutes on a note but adds three minutes of clicking around a new interface, you have failed the clinician." — Source: [The Heart of Healthcare]
- On feedback loops: "Clinician feedback is the oxygen that fuels product development. If they tell us a feature adds friction, we rip it out." — Source: [The 20 Minute VC]
- On aligning incentives: "When the workflow makes the doctor's day easier, adoption happens organically rather than as a top-down mandate." — Source: [Health Evolution]
- On legacy systems: "You can't replace the EHR overnight. You have to build elegant bridges that make the legacy systems vastly more efficient." — Source: [Pioneers of AI]
Part 6: Trust, Transparency, and Privacy
- On the foundation of trust: "In healthcare, trust is your only currency. If a physician cannot trace how the AI arrived at a conclusion, they will abandon the tool." — Source: [NEJM AI Grand Rounds]
- On verifiability: "We built our system so a doctor can click on any generated sentence and instantly hear the exact audio snippet it was drawn from." — Source: [This Week in Startups]
- On hallucination mitigation: "Generative AI can hallucinate, which is unacceptable in medicine. We constrain our models to strictly adhere to what was actually spoken in the room." — Source: [Digital Health Inside Out]
- On patient consent: "Patients are remarkably open to having their visits recorded if you explain that the technology is there to help the doctor focus entirely on them." — Source: [The Heart of Healthcare]
- On data stewardship: "We do not own the clinical data; we are simply stewards of it. Respecting patient privacy is the baseline requirement for operating in this space." — Source: [No Priors Podcast]
- On algorithmic bias: "We have to proactively train our models on diverse accents and vernaculars so that the technology works equally well for every patient demographic." — Source: [Abridge Blog]
- On transparent AI: "Black box models have no place in clinical decision-making. The software must explain its work." — Source: [Observer Interview]
- On regulatory compliance: "HIPAA compliance isn't a checklist; it's a fundamental architectural decision that dictates how you manage and secure audio data." — Source: [The 20 Minute VC]
- On clinical oversight: "The AI is an assistant, not an autonomous agent. The final review and signature must always belong to the human physician." — Source: [The 229 Podcast]
Part 7: Product-Market Fit in Health Tech
- On the desert of startup life: "Finding product-market fit in healthcare can feel like wandering in a five-year desert. The sales cycles are long and the bar for safety is incredibly high." — Source: [The 20 Minute VC]
- On solving real problems: "Don't build AI in search of a problem. Start with the most painful friction point in a doctor's day and engineer backward from there." — Source: [No Priors Podcast]
- On dual expertise: "Having clinical experience on the founding team isn't just a nice-to-have; it is an absolute necessity to navigate the nuances of medical workflows." — Source: [Digital Health Inside Out]
- On scaling too fast: "In healthcare, if you scale before the product is genuinely ready, you burn bridges with health systems that will take a decade to rebuild." — Source: [This Week in Startups]
- On the value proposition: "The return on investment for our platform is measured in reduced turnover, happier clinicians, and more accurate clinical documentation." — Source: [Health Evolution]
- On user obsession: "We spend an inordinate amount of time watching how doctors physically interact with their computers. That observation drives our roadmap." — Source: [The Heart of Healthcare]
- On building a team: "You need a culture that blends the urgency of a Silicon Valley tech company with the rigorous conservatism of a medical board." — Source: [Pioneers of AI]
- On capital strategy: "Raising money is a milestone, not the goal. The goal is deploying that capital to build infrastructure that fundamentally improves care." — Source: [The 20 Minute VC]
- On the inflection point: "When doctors tell you they would quit their jobs if you took the software away, you know you have achieved true product-market fit." — Source: [Observer Interview]
Part 8: The Future of Ambient Intelligence
- On the early innings: "We are still in the very early days of ambient AI in medicine. What we have now is just the foundation for what is possible over the next decade." — Source: [No Priors Podcast]
- On proactive care: "Eventually, conversational intelligence will move from documenting the past to proactively suggesting care pathways in real time." — Source: [The 229 Podcast]
- On patient empowerment: "If we capture the conversation accurately, we can generate a patient-facing summary that translates complex medical jargon into accessible language." — Source: [HLTH Conference]
- On continuous learning: "A health system with ambient AI running in every room becomes a massive, real-time learning engine for best clinical practices." — Source: [NEJM AI Grand Rounds]
- On reducing disparities: "By standardizing the quality of documentation and ensuring nothing is missed, AI can help close gaps in care equity." — Source: [Abridge Blog]
- On the invisible interface: "The ultimate goal is for the technology to disappear entirely into the background, leaving only the doctor and the patient." — Source: [Digital Health Inside Out]
- On clinical trials: "Ambient data capture will eventually streamline clinical trial enrollment by automatically identifying patients who meet complex criteria based on their clinic visits." — Source: [Health Evolution]
- On underhyped potential: "Despite all the noise around artificial intelligence, its long-term potential to transform the day-to-day reality of healthcare is actually underhyped." — Source: [This Week in Startups]
- On the legacy of AI in medicine: "If we do this right, the next generation of doctors will find it absurd that we used to spend hours manually typing notes after seeing patients." — Source: [Pioneers of AI]